
Blog
Hormone & Growth Support: Targeted Peptides & Hormones

Hormone regulation and growth support are foundational to human physiology, governing cellular metabolism, tissue repair, muscle growth, aging, and overall homeostasis. As physiological function naturally declines with age, or is disrupted by injury, stress, or metabolic imbalance, advanced hormone and peptide-based therapies have emerged as targeted solutions to restore optimal hormonal function, enhance growth processes, and mitigate age-related decline. This article provides a comprehensive, evidence-based overview of key compounds in the Hormone & Growth Support category—including peptides, recombinant hormones, and growth factors—exploring their molecular mechanisms, therapeutic applications, and clinical relevance for physiological optimization.
The Science of Hormone & Growth Support: Core Principles
Hormones and growth factors act as signaling molecules that regulate gene expression, cellular proliferation, differentiation, and repair across multiple organ systems. The growth hormone (GH)/insulin-like growth factor-1 (IGF-1) axis is central to these processes, orchestrating growth, metabolism, and tissue regeneration. Peptide therapies targeting this axis, along with other key hormones, offer distinct advantages over traditional hormone replacement therapy (HRT): they exhibit high specificity, minimal off-target effects, and the ability to modulate endogenous hormone production rather than simply replacing hormones—supporting physiological balance and reducing long-term risks.
This category encompasses three primary classes of compounds: growth hormone-releasing peptides (GHRPs), growth hormone-releasing hormones (GHRHs), recombinant hormones, and other supportive peptides/hormones—each with unique mechanisms to enhance hormone function and support growth.
Key Compounds for Hormone & Growth Support: Mechanisms and Clinical Applications
1. Growth Hormone-Releasing Peptides (GHRPs)
GHRPs are synthetic peptides that stimulate the secretion of endogenous growth hormone (GH) from the anterior pituitary gland by activating the ghrelin receptor (GHS-R1a). They act independently of the hypothalamic-pituitary-adrenal (HPA) axis, offering a targeted approach to boost GH levels without disrupting other hormonal pathways. Below are the key GHRPs in this category:
GHRP-2 Acetate
GHRP-2 Acetate is a synthetic hexapeptide (His-D-Trp-Ala-Trp-D-Phe-Lys-NH2) with high affinity for the GHS-R1a receptor. Its primary mechanism involves stimulating GH secretion via calcium influx into somatotroph cells of the pituitary, while also inhibiting somatostatin (the primary GH-inhibiting hormone). Unlike some GHRPs, GHRP-2 exhibits minimal appetite-stimulating effects (a common side effect of ghrelin agonists) and has a short half-life (approximately 30–60 minutes), requiring multiple daily administrations for sustained GH elevation.
Clinical applications include age-related GH deficiency, muscle wasting syndromes (e.g., cancer cachexia, post-surgical recovery), and metabolic optimization (improved lipid metabolism, reduced visceral fat). Preclinical studies demonstrate its ability to enhance lean muscle mass, accelerate tissue repair, and improve insulin sensitivity in aged models.
GHRP-6 Acetate
GHRP-6 Acetate is a synthetic hexapeptide (His-D-Trp-Ala-Trp-D-Phe-Lys-NH2) structurally similar to GHRP-2 but with a stronger appetite-stimulating effect, attributed to its potent activation of the ghrelin receptor. Like GHRP-2, it stimulates GH secretion by activating somatotroph cells and inhibiting somatostatin, but it also increases the release of prolactin and cortisol (albeit to a lesser extent than other GHRPs).
Its unique appetite-stimulating property makes it particularly valuable for individuals with cachexia, anorexia, or post-illness weight loss, while its GH-stimulating effects support muscle growth and tissue repair. It has a similar half-life to GHRP-2 (30–60 minutes) and is often used in combination with GHRHs to amplify GH release.
Ipamorelin
Ipamorelin is a pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) and a selective GHS-R1a agonist, distinguished by its exceptional safety profile and minimal side effects. Unlike GHRP-2 and GHRP-6, it does not significantly stimulate prolactin or cortisol secretion, making it ideal for long-term use and individuals sensitive to hormonal fluctuations. Its mechanism of action involves targeted activation of GHS-R1a, leading to dose-dependent GH secretion without disrupting the HPA axis.
Ipamorelin has a longer half-life (60–90 minutes) compared to other GHRPs, allowing for less frequent dosing. Clinical applications include age-related GH deficiency, anti-aging interventions, muscle preservation, and metabolic health (improved glucose tolerance and lipid profiles). It is also commonly combined with GHRHs to enhance synergistic GH release.

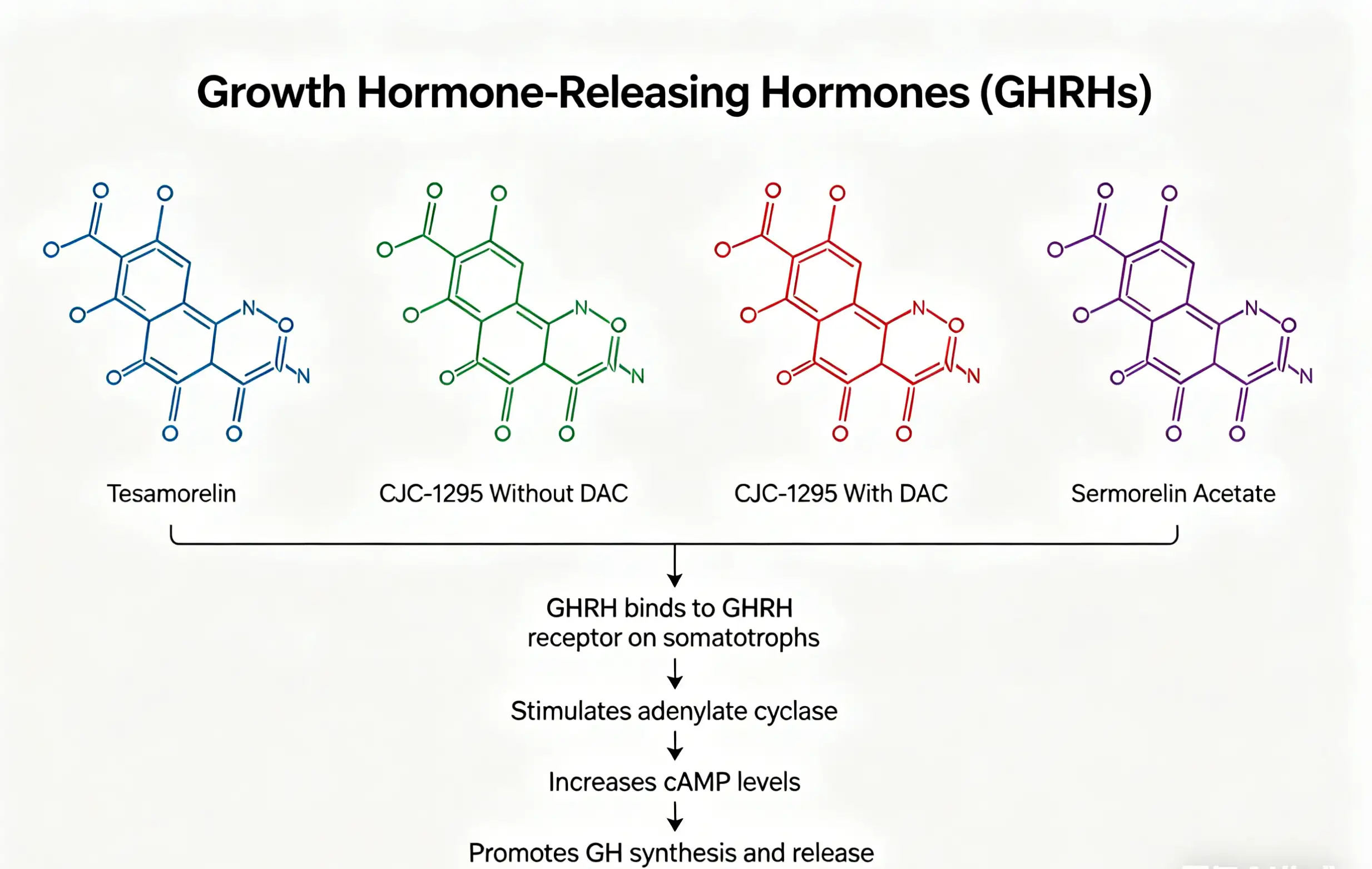
2. Growth Hormone-Releasing Hormones (GHRHs)
GHRHs are endogenous peptides that stimulate GH secretion by binding to GHRH receptors on the anterior pituitary. Synthetic GHRHs and their analogs offer sustained GH elevation by mimicking the body’s natural GHRH release, often used in combination with GHRPs to maximize synergistic effects.
Tesamorelin
Tesamorelin is a synthetic analog of human GHRH (1–44), modified to enhance stability and bioavailability. It acts by binding to GHRH receptors on somatotroph cells, stimulating GH secretion in a pulsatile manner (mimicking endogenous GH release), which is critical for maintaining physiological GH function. Unlike recombinant GH, Tesamorelin preserves the body’s natural feedback mechanisms, reducing the risk of overstimulation and side effects (e.g., acromegaly).
Clinically, Tesamorelin is approved for the treatment of HIV-associated lipodystrophy, as it reduces visceral adipose tissue (VAT) by enhancing GH-dependent lipolysis. It also has applications in age-related GH deficiency, improving lean muscle mass, bone density, and cognitive function. Its half-life (2–3 hours) allows for once-daily administration, making it a convenient option for long-term therapy.
CJC-1295 Without DAC
CJC-1295 Without DAC (Drug Affinity Complex) is a synthetic GHRH analog (modified at positions 2, 8, 15, and 27) designed to enhance GH secretion without the prolonged half-life associated with DAC-modified versions. It binds to GHRH receptors on the pituitary, stimulating pulsatile GH release, and has a half-life of approximately 30 minutes—similar to endogenous GHRH. This short half-life mimics the body’s natural GH secretion pattern, reducing the risk of desensitization and maintaining physiological balance.
It is often used in combination with GHRPs (e.g., Ipamorelin) to amplify GH release, making it ideal for short-term growth support (e.g., post-injury recovery, muscle building) and individuals seeking targeted GH elevation without prolonged exposure. Its rapid clearance minimizes systemic side effects, making it a well-tolerated option for clinical and research use.
CJC-1295 With DAC
CJC-1295 With DAC is a long-acting GHRH analog, modified with a Drug Affinity Complex (DAC) to extend its half-life to 8–10 days. This modification allows for sustained, low-level GH secretion over an extended period, eliminating the need for daily administration. Like CJC-1295 Without DAC, it binds to GHRH receptors, but its prolonged bioavailability results in consistent GH elevation, supporting long-term tissue repair, muscle growth, and anti-aging effects.
Clinical applications include chronic GH deficiency, age-related decline, and long-term regenerative therapy. However, its prolonged action requires careful monitoring to avoid overstimulation, as sustained GH elevation may increase the risk of insulin resistance or soft tissue overgrowth. It is often used as a long-term maintenance therapy, with dosing frequency ranging from once weekly to once every two weeks.
Sermorelin Acetate
Sermorelin Acetate is a synthetic fragment of human GHRH (1–29), the active portion of the endogenous hormone. It stimulates GH secretion by binding to GHRH receptors, with a mechanism identical to endogenous GHRH but with enhanced stability. It has a short half-life (15–30 minutes), requiring multiple daily administrations, but offers a highly physiological approach to GH elevation—mimicking the body’s natural pulsatile release.
Sermorelin is widely used in anti-aging medicine, age-related GH deficiency, and pediatric growth hormone deficiency (in some regions). It supports lean muscle mass, bone density, and metabolic health, with a favorable safety profile due to its physiological mechanism. It is often combined with GHRPs to enhance GH release and extend therapeutic effects.

3. Recombinant Hormones
Recombinant hormones are synthetically produced versions of endogenous hormones, designed to replace or supplement deficient hormone levels. They offer direct, potent effects but require careful dosing to avoid hormonal imbalance.
HGH (Human Growth Hormone)
HGH (Somatropin) is a recombinant form of human growth hormone, identical in structure to endogenous GH produced by the anterior pituitary. It acts directly on target tissues via GH receptors, regulating growth, metabolism, tissue repair, and immune function. Key effects include stimulation of IGF-1 production (a critical mediator of GH’s growth-promoting effects), enhanced protein synthesis, lipolysis (fat breakdown), and bone mineralization.
Clinical applications include pediatric growth hormone deficiency, adult GH deficiency, Turner syndrome, and Prader-Willi syndrome. It is also used off-label for anti-aging, muscle growth, and post-injury recovery, though long-term use requires monitoring for side effects (e.g., insulin resistance, acromegaly, joint pain). HGH is administered via subcutaneous injection, with dosing tailored to age, weight, and clinical indication.
HCG (Human Chorionic Gonadotropin)
HCG is a glycoprotein hormone produced naturally during pregnancy, with structural similarity to luteinizing hormone (LH). Its primary mechanism involves binding to LH receptors in the testes (males) and ovaries (females), stimulating testosterone production in males and ovulation in females. In the context of hormone & growth support, HCG is primarily used to preserve testicular function during exogenous testosterone therapy, preventing testicular atrophy by maintaining LH-like signaling.
It is also used in male infertility (to stimulate spermatogenesis) and female ovulation induction. HCG has a half-life of 24–36 hours, with administration via subcutaneous or intramuscular injection. Its use requires monitoring of testosterone and estrogen levels to avoid hormonal imbalance.
IGF-1 LR3 (Insulin-Like Growth Factor-1 Long R3)
IGF-1 LR3 is a long-acting analog of insulin-like growth factor-1 (IGF-1), modified at position 3 (arginine replaced with leucine) and extended with a 13-amino acid tail to enhance stability and bioavailability. Unlike endogenous IGF-1, which is primarily produced in the liver in response to GH, IGF-1 LR3 acts directly on target tissues (muscle, bone, skin) to stimulate cellular proliferation, protein synthesis, and tissue repair.
Its key advantages include a longer half-life (12–18 hours) compared to endogenous IGF-1 (1–2 hours) and resistance to binding proteins (IGFBPs), which normally reduce IGF-1 bioavailability. Clinical applications include muscle wasting, tissue repair, and GH resistance (where GH administration is ineffective). It is also used in research to study the role of IGF-1 in growth and aging, with careful monitoring due to potential insulin-like effects (e.g., hypoglycemia).
Clinical Considerations and Safety
While the compounds discussed offer significant therapeutic potential, it is critical to note that many remain research-grade or require clinical supervision. Key considerations include:
- Dosing Individualization: Hormone and peptide therapy must be tailored to age, weight, hormonal status, and clinical goals to avoid overstimulation or deficiency.
- Monitoring: Regular testing of GH, IGF-1, testosterone, cortisol, and glucose levels is essential to ensure safety and efficacy, particularly for long-term use.
- Contraindications: Compounds such as HGH and IGF-1 LR3 are contraindicated in individuals with active cancer, severe diabetes, or acromegaly. HCG should be avoided in pregnant individuals.
- Side Effects: Common side effects (e.g., injection site reactions, transient fatigue, mild hypoglycemia) are typically mild and dose-dependent, but severe side effects (e.g., acromegaly, insulin resistance) may occur with improper dosing.
Conclusion
Hormone & Growth Support therapies represent a sophisticated approach to physiological optimization, leveraging the specificity of peptides and the potency of recombinant hormones to restore hormonal balance, enhance growth, and mitigate age-related decline. From GHRPs (Ipamorelin, GHRP-2, GHRP-6) and GHRHs (Tesamorelin, CJC-1295, Sermorelin) to recombinant hormones (HGH, HCG, IGF-1 LR3), each compound offers unique mechanisms to support cellular function, tissue repair, and metabolic health.
The synergistic formulation of CJC-1295 Without DAC and Ipamorelin further exemplifies the power of combined peptide therapy, offering targeted, physiological GH elevation with minimal side effects. As research continues to advance, these therapies are poised to play an increasingly critical role in anti-aging medicine, regenerative therapy, and the management of hormonal deficiencies—empowering individuals to optimize their health and quality of life.